Introduction
Healthcare front desks are under constant pressure. Scheduling calls, prescription refill requests, billing questions, insurance verification — the volume never stops, and staff are stretched thin. The result is predictable: long hold times, frustrated patients, and burned-out staff spending their days answering the same five questions on repeat.
The instinctive response is to hire more people. That approach adds headcount without fixing the underlying bottleneck.
A smarter path is using technology to route patients to the right resource faster, handling routine requests automatically while preserving human attention for the calls that genuinely need it. Automated call routing doesn't replace your team. It takes the low-complexity, high-volume work off their plates.
This guide covers how the technology works, which routing strategies drive real results, what HIPAA compliance requires, and a practical roadmap for getting started. Healthcare organizations evaluating after-hours coverage can See How AI Handles After-Hours Calls to see a real-time example before reading further.
Key Takeaways
- Appointments and prescription refills drive most inbound call volume — and the clearest ROI for automation
- Modern AI routing uses natural language processing: patients describe their need in plain speech, no "press 1" menus required
- Healthcare data breaches average $7.42M per incident; HIPAA compliance and a signed BAA are mandatory, not optional
- Tampa General's AI routing cut ambulatory wait times by 58% and increased daily appointments scheduled by 17%
- Start with one or two high-volume workflows, measure against baseline handle-time or abandonment-rate benchmarks, then expand
What Is Automated Call Routing in Healthcare?
Automated call routing uses technology — IVR, AI, natural language processing — to direct incoming patient calls to the right department, staff member, or self-service option. No human operator required to make that routing decision. In healthcare, a misrouted call isn't just a minor inconvenience; it can delay a prescription refill, push back a referral, or leave a patient in the wrong queue when they needed urgent guidance.
The call types this applies to are broad:
- Appointment scheduling and rescheduling
- Prescription refill requests
- Billing and insurance questions
- After-hours triage and on-call access
- Lab result inquiries and general FAQs
The scale of the problem is real. A peer-reviewed study of The Urology Group — a 43-provider, 12-location outpatient practice — recorded 299,028 answered calls over the study period, averaging 5,751 calls per week. Earlier research from Mercy Hospital's primary care practices found that appointments plus prescription refills alone accounted for 67% of incoming patient calls — meaning two-thirds of call volume is largely routine and repeatable.

That volume of routine, repeatable calls is exactly where automation earns its place — though with one critical boundary: automated routing does not replace clinical judgment. It should never handle complex care coordination, emotional crises, or conversations requiring medical decision-making. Those calls need a human. The goal is to protect that human capacity by automating everything else.
How the Technology Works: From IVR to Conversational AI
Traditional IVR: The Foundation
Interactive Voice Response is the "press 1 for appointments, press 2 for billing" system most patients already know — and frequently dread. IVR is inexpensive and reliable for simple call segregation, but the limitations are real. Rigid menu trees frustrate callers who can't find the right option. Patients who reach the wrong department hang up or wait through another queue. And IVR can't adapt when someone says something unexpected.
Research from VHA call centers found that longer average speed of answer (ASA) was directly associated with worse patient perceptions of urgent-care access — evidence that telephone friction has real clinical consequences, not just satisfaction scores.
Conversational AI and NLP: The Upgrade
Modern systems replace rigid menus with Natural Language Processing (NLP) — the technology that lets a machine understand human speech as it's actually spoken. Instead of navigating a five-level menu, a patient says: "I need to reschedule my Thursday appointment with Dr. Johnson." The system understands the intent, confirms the request, and routes accordingly.
According to HIMSS, NLP derives computable, actionable data from natural human language — and Natural Language Understanding (NLU) adds reasoning and semantic inference on top of that. Together, they allow routing systems to handle the messy, unpredictable ways real patients actually communicate.
Two additional capabilities push this further:
- Machine learning analyzes historical call patterns — caller ID, time of day, call reason, prior interactions — and continuously refines routing decisions with every call, no manual reprogramming required.
- Sentiment analysis detects emotional signals in the caller's voice (distress, frustration, urgency) and flags those calls for prioritized handling or escalation to agents trained for sensitive interactions.
Platforms like Eva Speaks bring these capabilities together through LLM integration, real-time AI processing, and customizable call-flow scripts — allowing healthcare practices to configure routing logic that reflects their specific workflows, office hours, and patient populations.
The evidence for this model's effectiveness is concrete. Tampa General Hospital replaced traditional menu routing with conversational AI integrated with Epic, Cisco, and SpinSci — achieving a 56% reduction in ambulatory queue abandonment, 58% lower wait times for ambulatory scheduling, and a 17% increase in average daily appointments scheduled. You can Watch AI Call Flow Demo to see how an AI-powered routing conversation unfolds in a healthcare context.

Core Routing Strategies That Drive Results
Skill-Based and Empathy-Driven Routing
Skill-based routing matches the incoming call to the agent best equipped to handle it — not simply the next available person. A patient calling about a cardiology billing dispute goes to a billing specialist with cardiology experience. A Spanish-speaking patient gets routed to a bilingual staff member without having to ask.
This directly affects First Call Resolution (FCR). The Healthcare Financial Management Association lists 100% first contact resolution as a target standard for healthcare clients. Stanford's Clinical Advice Services reached a related benchmark: 92% of patients had all needs met during a single call, with fewer than 10% of primary care calls requiring physician escalation.
Empathy-driven routing takes skill-based logic one step further. When sentiment analysis detects a distressed or anxious caller, the system routes them to agents trained for sensitive conversations rather than the standard queue. That same logic extends beyond business hours, where routing gaps tend to be most costly.
After-Hours and On-Call Routing
After-hours coverage is where many healthcare organizations have the most acute gaps. Without automated routing, after-hours calls either go unanswered or burden on-call physicians unnecessarily. The AMA reported that Stanford's legacy system routed after-hours calls directly to attending physicians, contributing to burnout — a problem the redesigned routing model substantially reduced by adding triage layers before escalation.
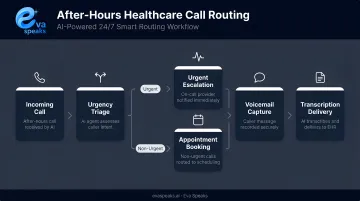
A modern after-hours routing system can:
- Direct urgent calls to an on-call nurse line or physician queue
- Route routine requests (appointment scheduling, FAQs) to an AI voice agent
- Transcribe voicemails so staff can triage messages by reading rather than listening through a queue
- Escalate calls showing signs of clinical urgency to a live on-call resource
Multilingual and Accessibility Routing
U.S. Census data shows 21.7% of U.S. residents age 5 and older speak a language other than English at home, with 61.1% of non-English speakers using Spanish. A routing system without a language selection option creates access barriers before the first word is spoken.
Multilingual IVR and AI routing lets patients select their preferred language at call start, routing them directly into the appropriate language pathway. For organizations subject to Title VI requirements, this is also a compliance consideration, not just a service quality one.
Smart Queue Management
When call volume spikes, queue management tools prevent abandonment:
- Virtual Hold Callback: saves the caller's place and calls them back when an agent is available, eliminating hold time entirely
- Call-to-Text Deflection: moves simple requests to a text channel, freeing up voice queues for calls that need them
- HIPAA-Compliant Voicemail Transcription: converts voicemails to readable text so staff can triage by priority, not by timestamp
EHR Integration, HIPAA Compliance, and the Patient Journey
EHR Integration: Closing the Loop
Routing a call to the right agent is only half the job. When the call routing system connects to the Electronic Health Record, appointment bookings or changes made during the call update the EHR automatically — no double entry, no clerical errors introduced by manual transcription. CRM integration adds another layer: Screen Pop surfaces the patient's record on the agent's screen the moment the call connects, so the agent already knows who's calling and why before saying hello.
Tampa General's implementation demonstrated this in practice — their AI agent authenticated callers, retrieved real-time scheduling data from Epic, and completed transactions without manual intervention.
One governance caution from VHA research: centralized routing systems that generate excessive EHR alerts can increase provider workload rather than reduce it. How integration is designed matters as much as whether it exists.
HIPAA Compliance: What Platforms Must Provide
Any platform handling Protected Health Information (PHI) — which includes voice recordings, transcripts, scheduling data, and caller identification in a healthcare context — must meet specific requirements:
- Data encryption in transit and at rest
- Role-based access controls limiting PHI access to authorized staff
- Audit logging to track who accessed what and when
- Signed Business Associate Agreement (BAA) with the vendor, as required by HHS Office for Civil Rights
The financial stakes are significant. According to IBM's 2025 Cost of a Data Breach report, the healthcare industry averages $7.42 million per breach — the highest of any sector. That figure makes compliance a core risk management decision, not an administrative formality.
When evaluating vendors, ask directly: Are you HIPAA-compliant? Do you offer a BAA? What encryption standards do you use? If those questions don't get clear answers, keep looking. For Eva Speaks specifically, prospective healthcare clients should contact the team at privacy@evaspeaks.ai to discuss compliance documentation and BAA availability.
Omnichannel Continuity: No More Repeating Yourself
Solid compliance infrastructure supports the back end. The patient experience, though, depends on what happens across every touchpoint — and patients rarely stick to one channel.
A routing system that treats each channel as isolated forces patients to repeat themselves every time they switch, one of the fastest ways to erode satisfaction. Omnichannel journey orchestration maintains context across touchpoints, so a patient who started a conversation via text and follows up by phone doesn't have to re-explain their situation from scratch.
Common channels that need continuity:
- Phone calls routed to the appropriate department or agent
- SMS/text threads tied to the patient's existing record
- Patient portal messages that carry context into live calls
- Email inquiries that trigger the correct follow-up workflow
Healthcare organizations that want to discuss how to design omnichannel continuity for their specific patient population can Talk to an AI Communication Expert.
Measuring Performance: The KPIs That Matter
Tracking the right metrics is what separates an automated routing implementation that improves over time from one that stagnates.
Core KPIs for healthcare call routing:
| KPI | Healthcare Benchmark |
|---|---|
| Average Speed of Answer (ASA) | ≤30 seconds (VHA target) |
| Call Abandonment Rate | ≤5% (VHA target) |
| First Call Resolution (FCR) | 100% target (HFMA guidance) |
| Average Handle Time (AHT) | ~3:41 (Urology Group internal benchmark) |
| Daily appointments scheduled | Track week-over-week vs. baseline |
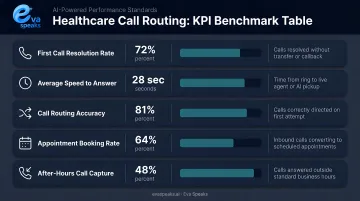
FCR and ASA are your two most diagnostic metrics. FCR captures whether the patient's actual need was resolved — not just whether someone answered. Longer ASA, by contrast, has been directly linked in peer-reviewed research to worse patient perceptions of urgent-care access. Together, they tell most of the story.
Modern AI routing platforms collect data from every interaction — peak call times, most common call reasons, where callers drop out of IVR menus — and surface those patterns through analytics. That data directly informs staffing decisions, menu redesigns, and workflow changes. Unlike static systems, AI-powered platforms refine their intent recognition and routing accuracy with each call — no manual reprogramming required. Over time, that compounding accuracy is what drives measurable cost and efficiency gains.
Your Implementation Roadmap
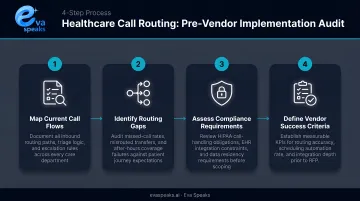
Phase 1: Audit Before You Buy
Before selecting any platform, get clear on what you're actually trying to solve:
- Audit current call volume — track total inbound calls for 30 days and tag by reason (scheduling, refills, billing, etc.)
- Identify your top 5-7 call types — these are your automation candidates
- Separate routine from complex — scheduling, FAQs, and refill routing are automation-ready; clinical triage and lab result discussions are not
- Set target benchmarks — define your ASA goal, abandonment rate target, and FCR objective before go-live
Phase 2: Vendor Selection Criteria
Healthcare is not a generic use case. Evaluate vendors specifically on:
- HIPAA compliance with BAA availability — confirm, don't assume
- EHR and practice management integration — what systems connect, and what does the integration actually do?
- Natural language capability — can it handle how your patient population actually speaks, including healthcare-specific phrasing?
- Multilingual support — especially if you serve Spanish-speaking patients
- Customizable routing rules — can you configure workflows to match your specific departments and protocols?
Platforms that combine LLM integration with customizable call-flow scripts — like EvaSpeaks — handle the variable routing needs of healthcare practices more effectively than legacy IVR systems built around fixed menus. EvaSpeaks also represents a low-infrastructure-dependency option: it connects to existing telephony through standard integrations rather than requiring hardware changes or a new phone system, which reduces the barrier to adoption for practices that don't want a large IT project as part of their call routing upgrade.
Here is how the two approaches compare across the dimensions that matter most for healthcare practices evaluating a routing upgrade:
| Traditional IVR | EvaSpeaks (AI-Powered) | |
|---|---|---|
| Features | Fixed menu trees, DTMF key-press navigation, basic call transfer | Natural language understanding, intent detection, sentiment analysis, real-time EHR integration |
| Best-fit Business Size | Large health systems with dedicated IT teams and legacy PBX infrastructure | Solo practices to mid-size multi-location groups; scales without added IT overhead |
| Key Strengths | Predictable, battle-tested for simple call segregation | Flexible scripting, continuous learning, handles unpredictable patient language |
| Implementation Complexity | High - requires PBX configuration, custom integrations, and IT project management | Low - connects to existing telephony via standard integrations; no hardware changes |
| Integration Capability | Limited; typically requires custom middleware to connect with EHR/CRM | Native integrations with EHR systems and CRMs; screen-pop and real-time data retrieval out of the box |
Phase 3: Phased Rollout
Don't automate everything at once. Start narrow, prove the model, then expand:
- Week 1–4: Deploy on one high-volume, low-complexity workflow (appointment scheduling or after-hours routing)
- Week 5–8: Measure results against your benchmarks; gather staff feedback on call quality and routing accuracy
- Week 9–12: Refine routing logic based on data; add a second workflow
- Ongoing: Track ASA, abandonment rate, and FCR monthly — these numbers tell you when a workflow is ready to scale and when it needs adjustment
Healthcare organizations ready to begin that phased rollout can Get a Customized Workflow Recommendation to map the right workflows to their specific call volume and practice size.
Frequently Asked Questions
What is automated call routing?
Automated call routing uses technology — IVR, AI, and NLP — to direct incoming calls to the right person, department, or self-service option without a manual operator. In healthcare, this means patients reach the correct resource faster, reducing hold times and preventing misroutes that delay care.
What is the difference between call routing and IVR?
IVR is one tool within call routing: the traditional "press 1" menu system. Call routing is the broader strategy, which today also includes conversational AI that understands natural speech and routes calls based on intent, sentiment, and patient history without requiring menu navigation.
What are the four basic methods of call routing?
The four core approaches are:
- Time-based routing — directs calls based on business hours or time of day
- Skill-based routing — matches callers to agents by expertise
- Queue-based routing — connects to the first available agent in priority order
- AI/predictive routing — uses historical data and intent analysis to match callers to the optimal resource
Is automated call routing in healthcare HIPAA compliant?
Compliant solutions exist, but compliance must be verified, not assumed. Any vendor handling PHI must provide data encryption, access controls, audit logging, and a signed Business Associate Agreement (BAA). HIPAA compliance is a vendor selection requirement, not a default feature.
How does automated call routing reduce patient wait times?
By routing calls to the right destination on the first attempt, offering callback options so patients don't sit on hold, and enabling AI to handle routine inquiries without queuing, automated systems reduce total time to resolution. Tampa General's implementation cut ambulatory scheduling wait times by 58%.
What is the ROI of automating call routing in a medical practice?
ROI comes from reduced staff time on repetitive calls, lower abandonment rates, and fewer missed appointments — HFMA estimates no-shows cost providers $150 billion annually. The Urology Group's centralized model cut operating expenses by 7.7% while improving speed of answer, offering a concrete benchmark for outpatient planning.